|
|
Triage is the process through which EMS providers rapidly identify life threatening injuries and sort casualties according to treatment priority. Triage, though applied differently and involving various algorithms, is designed to impart a sense of order upon an otherwise uncontrolled situation. In the prehospital arena, it enables EMTs and paramedics to direct their care and resources so that the the greatest benefit can be achieved for the greatest number of casualties. A triage process can be applied to any incident that threatens to exceed the capabilities of any EMS agency or responder. A serious multiple vehicle collision could rapidly overwhelm a single ambulance's resources, and a triage paradigm assists paramedics with sorting the injured according to severity. A successful triage method is one that is rapidly applied, easily remembered, and accurately reflects the magnitude of an underlying injury. Though several triage methods exist, all of them are are similar in purpose. Hemodynamically unstable patients are usually designated as a "high priority," while patients who are capable of obeying commands or ambulating without assistance are classified as a lower treatment priority. Triage methods commonly utilize color coded tags, mats, or ribbons so that patients can physically be "labeled" with important information such as triage category or vital signs. Some definitions are helpful in the study of mass casaulty care and the triage process:
SAMPLE TRIAGE PROCESS
SAMPLE TRIAGE PROCESS
- Ambulance 1 arrives at the scene of a mass casualty incident.
- The scene is deemed safe; the two responders exit their response vehicle and see at least two dozen people in need of attention
- The crew retrieves their triage equipment, requests additional assistance, and begins the process of triage
- Only life saving interventions (LSI) are performed during the triage process
- Rescuer 1 asks patients capable of ambulating to walk to a "GREEN" zone
- Rescuer 2 moves rapidly from patient to patient and applies color coded tags
- After several minutes, Rescuer 1 provides dispatch with an updated scene size up
- While waiting for additional resources, both rescuers re-assess the wounded
HELPFUL DEFINITIONS
Life Saving Interventions:
Interventions or procedures that, when rapidly applied, have the ability to correct a potential life threat. LSI's include: airway repositioning, tourniquet application, and needle decompression
Mass Casualty Incident (MCI):
An incident that temporarily overwhelms the capabilities of emergency medical responders. Typically EMS agencies have policies to delineate the specific number of casualties which would qualify for designation as a mass casualty incident
Disaster:
The precise definition of this term varies. The Federal Emergency Management Agency defines as [major] disaster as a natural event which cripples the emergency response infrastructure and requires mobilization of federal resources. On the more local level, a disaster occurs when the local emergency medical response apparatus cannot effectively mitigate the impact of the event upon the population.
Triage:
The term is derived from the French verb trier which means to separate or sort. It is an organized process through which injured patients are sorted according to their severity of illness. This process can have significant implications on the order of transport and the determination of hospital destination
Life Saving Interventions:
Interventions or procedures that, when rapidly applied, have the ability to correct a potential life threat. LSI's include: airway repositioning, tourniquet application, and needle decompression
Mass Casualty Incident (MCI):
An incident that temporarily overwhelms the capabilities of emergency medical responders. Typically EMS agencies have policies to delineate the specific number of casualties which would qualify for designation as a mass casualty incident
Disaster:
The precise definition of this term varies. The Federal Emergency Management Agency defines as [major] disaster as a natural event which cripples the emergency response infrastructure and requires mobilization of federal resources. On the more local level, a disaster occurs when the local emergency medical response apparatus cannot effectively mitigate the impact of the event upon the population.
Triage:
The term is derived from the French verb trier which means to separate or sort. It is an organized process through which injured patients are sorted according to their severity of illness. This process can have significant implications on the order of transport and the determination of hospital destination
SAMPLE TRIAGE SYSTEM PRESENTATION
The Maryland Institute for Emergency Medical Services Systems (MIEMSS) created a powerpoint presentation that reviews key aspects of a prehospital triage program. Using a common algorithm such as JumpSTART, MIEMSS deploys tags and other identifiers to assist with the orderly treatment, transport, and routing of mass casualty victims. The powerpoint presentation effectively describes the different triage categories and the process through which EMS would communicate specific patient needs to receiving facilities.
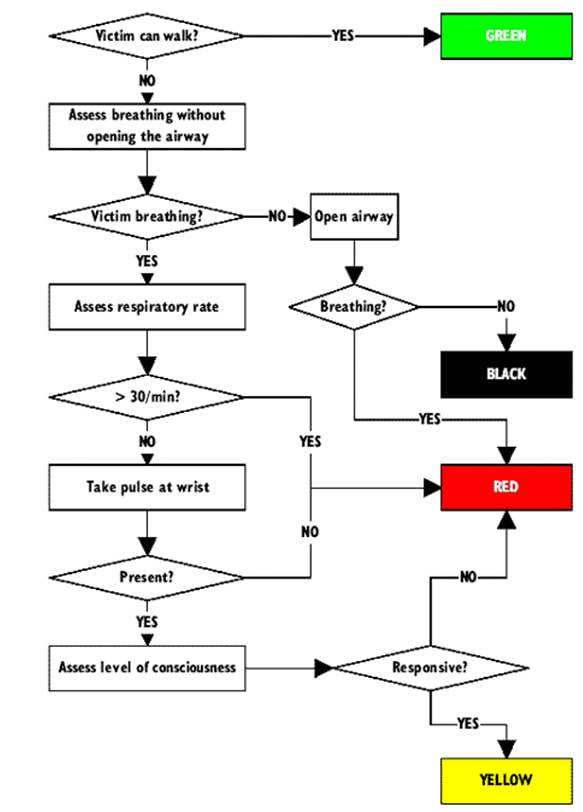
START (Simple Triage and Rapid Treatment) ALGORITHM
The START tool is one of the most widely utilized schemes for sorting out casualties. It consists of a basic initial assessment that follows with an evaluation of breathing, circulatory, and mental status. Ideally, the START triage assessment can be completed within one minute of encountering a casualty. It is not easy to rapidly sort through casualties and determine the relative severity of injury within seconds of encountering a patient. This challenge is precisely why triage schemes are developed. Effective paradigms assist clinicians with sorting out casualties into specific categories in order to maintain order and deliver potentially life saving care to patients most likely to benefit.
The Maryland Institute for Emergency Medical Services Systems (MIEMSS) created a powerpoint presentation that reviews key aspects of a prehospital triage program. Using a common algorithm such as JumpSTART, MIEMSS deploys tags and other identifiers to assist with the orderly treatment, transport, and routing of mass casualty victims. The powerpoint presentation effectively describes the different triage categories and the process through which EMS would communicate specific patient needs to receiving facilities.
START (Simple Triage and Rapid Treatment) ALGORITHM
The START tool is one of the most widely utilized schemes for sorting out casualties. It consists of a basic initial assessment that follows with an evaluation of breathing, circulatory, and mental status. Ideally, the START triage assessment can be completed within one minute of encountering a casualty. It is not easy to rapidly sort through casualties and determine the relative severity of injury within seconds of encountering a patient. This challenge is precisely why triage schemes are developed. Effective paradigms assist clinicians with sorting out casualties into specific categories in order to maintain order and deliver potentially life saving care to patients most likely to benefit.
START WALKTHROUGH AND CATEGORIES OF INJURY
One immediately helpful way to gauge the relative severity of injury is to ask patients if they are able to walk. The ability to ambulate denotes preserved mental and functional capacity. Patients able to obey commands and ambulate without assistance are immediately tagged as, "MINOR" or "GREEN." Green patients represent less severe injury patterns.
Patients unable to obey commands require further assessment. The next step in the (START) triage process is to assess effective breathing patterns. If the patient has no spontaneous respiratory effort, an attempt is made at repositioning the airway. If a jaw-thrust or similar airway maneuver does not result in respiration, the patient tagged as, "BLACK" or dead. Those there may be patients who are "black-tagged" and have a concurrent pulse, it is unlikely that these patients will survive without additional interventions. In a disaster setting, rescuers are encouraged to assess those patients most likely to benefit from emergent treatment. When resources are limited and there are potentially dozens- or hundreds more- patients to evaluate, there is not sufficient time to spend treating a patient with a potentially moribund injury.
There is a pediatric-specific modification to the START process called, "JumpSTART." The pediatric process incorporates the delivery of rescue breaths and some additional assessment components in order to more accurately tailor the initial triage decision.
Patients with impaired mental status or respiratory failure are "RED" tagged for "IMMEDIATE" treatment. The red triage category designates those patients who are likely to die if emergent treatment is delayed. Patients with a respiratory rate of > 30 per minute, altered perfusion, or decreased mental status are in need of immediate transport and stabilization. This category of patients may also require those "Life Saving Interventions" mentioned earlier such as: bleeding control, needle decompression, and airway stabilization.
The "IMMEDIATE," or "YELLOW" triage category is reserved for patients with injury patterns in need of urgent treatment. These patients may have broken bones, severe wounds, or other conditions that require urgent intervention. Under the START algorithm, a patient with delayed capillary with an intact mental status can be placed in the delayed category. Other conditions likely to fall into the "IMMEDIATE" or "YELLOW" category include: broken bones and respiratory distress.
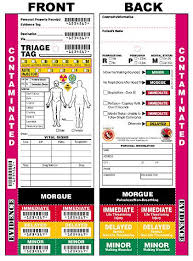
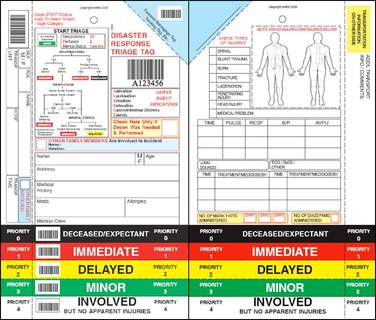
Triage tags are utilized to communicate these injury categories to clinicians tasked with mass casualty response and treatment. It is important to remember that categories are dynamic. Once the triage team is "caught up" and able to perform a reassessment, they can re-classify patients up and down the spectrum of triage acuity. Triage tags and color coded triage tarps are instrumental in providing clinicians with rapidly available information about the number and location of casualties in need of immediate treatment.
Note that the triage tag contains limited space for documentation related to injury, vital signs, and demographics. Some tags are bar-coded to facilitate integration with an EMS agency's electronic medical record. Typically, the color-coded portion of the tag can be removed/highlighted to indicate the specific triage category.
One immediately helpful way to gauge the relative severity of injury is to ask patients if they are able to walk. The ability to ambulate denotes preserved mental and functional capacity. Patients able to obey commands and ambulate without assistance are immediately tagged as, "MINOR" or "GREEN." Green patients represent less severe injury patterns.
Patients unable to obey commands require further assessment. The next step in the (START) triage process is to assess effective breathing patterns. If the patient has no spontaneous respiratory effort, an attempt is made at repositioning the airway. If a jaw-thrust or similar airway maneuver does not result in respiration, the patient tagged as, "BLACK" or dead. Those there may be patients who are "black-tagged" and have a concurrent pulse, it is unlikely that these patients will survive without additional interventions. In a disaster setting, rescuers are encouraged to assess those patients most likely to benefit from emergent treatment. When resources are limited and there are potentially dozens- or hundreds more- patients to evaluate, there is not sufficient time to spend treating a patient with a potentially moribund injury.
There is a pediatric-specific modification to the START process called, "JumpSTART." The pediatric process incorporates the delivery of rescue breaths and some additional assessment components in order to more accurately tailor the initial triage decision.
Patients with impaired mental status or respiratory failure are "RED" tagged for "IMMEDIATE" treatment. The red triage category designates those patients who are likely to die if emergent treatment is delayed. Patients with a respiratory rate of > 30 per minute, altered perfusion, or decreased mental status are in need of immediate transport and stabilization. This category of patients may also require those "Life Saving Interventions" mentioned earlier such as: bleeding control, needle decompression, and airway stabilization.
The "IMMEDIATE," or "YELLOW" triage category is reserved for patients with injury patterns in need of urgent treatment. These patients may have broken bones, severe wounds, or other conditions that require urgent intervention. Under the START algorithm, a patient with delayed capillary with an intact mental status can be placed in the delayed category. Other conditions likely to fall into the "IMMEDIATE" or "YELLOW" category include: broken bones and respiratory distress.
Triage tags are utilized to communicate these injury categories to clinicians tasked with mass casualty response and treatment. It is important to remember that categories are dynamic. Once the triage team is "caught up" and able to perform a reassessment, they can re-classify patients up and down the spectrum of triage acuity. Triage tags and color coded triage tarps are instrumental in providing clinicians with rapidly available information about the number and location of casualties in need of immediate treatment.
Note that the triage tag contains limited space for documentation related to injury, vital signs, and demographics. Some tags are bar-coded to facilitate integration with an EMS agency's electronic medical record. Typically, the color-coded portion of the tag can be removed/highlighted to indicate the specific triage category.